


This article requires a subscription to view the full text. If you have a subscription you may use the login form below to view the article. Access to this article can also be purchased.
- Address for Correspondence: Jeanne M. Isabel
, School of Health Studies, Northern Illinois University, DeKalb, IL, jisabel{at}niu.edu
ABSTRACT
This research included diabetes screening assessment for a population in Belize that may not have ready access to testing. Data gathered on gender, age, and ethnicity were correlated with measurement of waist circumference and hemoglobin A1c (HbA1c). The investigator used a point-of-care screening test for HbA1c to determine whether individuals fell within the normal range, the prediabetes range, or the diabetic range. A random selection of participants from the Belmopan region were tested. Analysis of the data indicated that 33.1% of the population tested in the prediabetes range for HbA1c. This percentage should be a concern to health care personnel in Belize who may have limited resources for patients’ diabetes treatment. An equally concerning finding is the number of participants in the diabetes range, 8.5% of whom had not been previously diagnosed. Diabetes education and screening is essential to the health and well-being of the people of Belize.
INTRODUCTION
A study of the prevalence of diabetes in 6 Central American countries was carried out by The Central America Diabetes Initiative and published in Diabetes Care in April 2012.1 This article reported that the prevalence of diabetes in Belize is higher than other Central American countries. Of all the noncommunicable diseases in the world, diabetes constitutes a major concern, especially in countries where diagnosis and treatment are not readily available. According to the 2015 report from the International Diabetes Federation, approximately 415 million adults have diabetes; by 2040, the number will rise to 642 million. The regions of South and Central America account for more than 20 million people with diabetes.2
In some countries with limited resources, awareness of potential diabetes risk is missing. The 2015 World Health Organization report for Belize listed diabetes as the number 2 cause of death in 2012, at 8.9% of the population. This statistic is just under the number 1 cause of death, ischemic heart disease, at 10.4%.3 A Centers for Disease Control and Prevention fact sheet for Belize, published in November 2013, listed diabetes as one of the top 10 causes of death.4 The risk for type 2 diabetes, which is often seen in middle-aged and older adults, increases among individuals who are overweight and inactive.5 An effort to raise awareness of diabetes within the country has resulted in an annual Diabetes Summit, held in the month of November in correlation with World Diabetes Day. The Diabetes Summit held in Belmopan, Belize on November 10, 2016, included a variety of speakers and presentations by health care representatives and high school youth associated with Youth for World Peace Wellness Ambassadors. Coordinated by a diabetes advocate in Belize, support for the Summit was solicited from agencies within the country, and free hemoglobin A1c (HbA1c) screening testing was offered. HbA1c screening was endorsed by the American Diabetes Association (ADA) in 2010 as a test for prediabetes and diagnosis of diabetes.6 Emphasis on awareness and prevention through healthy lifestyles was the theme for the 2016 Summit, which provided an opportunity to screen a variety of participants as part of this pilot research study.
Zakowski7 states that successful diabetes treatment relies on early diagnosis and accurate monitoring. Determination of risk factors in different parts of the world and prevalence of diabetes is valuable information to collect. This research intervention provided screening assessment to a population in Belize that may not have ready access to prediabetes testing. Data gathered on gender, age, and ethnicity, along with screening tests, may provide guidance for health care providers within the country. A point-of-care screening test for HbA1c was used to determine whether individuals fell within the normal, prediabetes, or diabetic range. This test has been determined to be a valuable tool to identify prediabetes.8 Participants included Belizeans between the ages of 20 and 70 who were randomly recruited through informational flyers. The HbA1c value, along with waist circumference and blood pressure measurements, provided valuable information for patient education.
Research questions posed for this population include the following: is there a link between gender and prediabetes? Is there a link between ethnicity and prediabetes? Is there a dominating gender or age group at risk? Is there a correlation among high blood pressure, waist circumference, and prediabetes? The premise of this research is to identify prediabetes in a population that can benefit from education programs. This pilot study resulted in data collection from 36 individuals. Preliminary analysis of data from this group indicated a significant need for additional testing, which took place in June 2017.
MATERIALS AND METHODS
Participants were recruited for the pilot study in November 2016 through distribution of an informational flyer advertising the free screening and speakers for the Diabetes Summit. Students from a local high school were also invited to attend the presentations. The June 2017 participant recruitment resulted from networking efforts by a diabetes advocate in Belize and agencies who supported the November 2016 Diabetes Summit. Dates and times for the screening in Belmopan and Belize City were organized through the supporting agencies whose employees were excited to be invited to participate.
Institutional review board approval was granted by Northern Illinois University, and each participant was asked to complete registration information and sign a consent form. The registration information, including phone number and email address, was collected to follow up with the participant if necessary. Participant age, gender, and ethnicity were recorded, along with a question of whether the participant had a previous diagnosis of diabetes. Measurements were made of waist circumference, blood pressure, and HbA1c.
Waist circumference was measured in inches with a cloth tape measure, using the recommended technique for waist measurement given by the ADA.9 Blood pressure measurements were performed using an automatic digital arm blood pressure monitor with pressure cuff.10 The HbA1c measurement was performed with capillary blood collected by fingerstick on a point-of-care device, A1cNow®+, following manufacturer recommendations.11 Quality control for the HbA1c was established using 2 levels of controls tested on each reagent lot. All materials for testing, including biohazard bags for waste disposal, were transported to Belize from the United States.
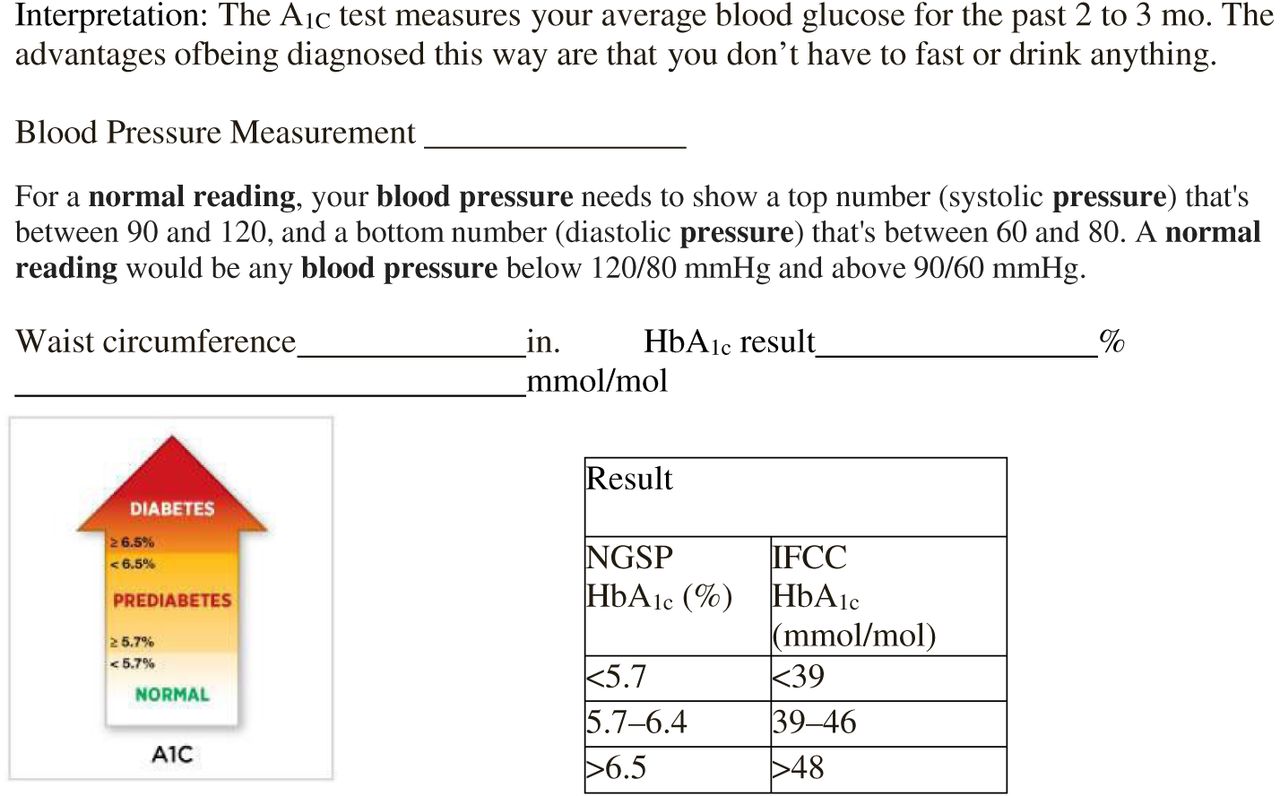
Once all measurements were completed, a result form was given to each participant with interpretation information (Figure 1). In addition to receiving results, each participant met with a nurse trained in Belize to address any questions and discuss possible diet or behavior changes for those individuals in the prediabetes risk zone.

Patient education information.
Setting
Belize is a country with a very culturally diverse population. Gathering data related to ethnicity may provide valuable answers to the research questions. There were 6 cultural categories identified: Creole, Mestizo, Garifuna, Maya, East Indian, and other.12 The group identifying themselves as Creole stem from ancestors of both African and European descent.
The Mestizo group identify with descendants from Spanish and Mayan cultures. The Mayan people of Belize have a rich history of religion and culture, with temple sites that are prominent tourist attractions. The group of people identifying themselves as Garifuna are descended from a mixture of African and Caribbean colonists. The East Indian group identify with descendants of Indian immigrants. The last group of other, made up of Nigerian, Hispanic, Chinese, and other African ethnicities, did not identify with any of the previous categories.
At the November 2016 Diabetes Summit, the screening and speaker sessions took place at the George Price Center in Belmopan, Belize. A table for testing and additional tables for registration and consulting were set up. High school students from the Youth for World Peace Ambassadors organization assisted with the registration and waist measurements. Two Belizean nurses assisted with patient education. Data from 36 participants were analyzed.
The second round of data collection, in June 2017, took place at designated employment agencies in Belmopan and Belize City. The organizations provided a conference roomthat was set up for the measurements, with registration and signing of consent forms taking place outside of the conference room. The following agencies in the community hosted the screening for their employees: Social Security Human Resources Office, Belize Natural Energy, Belize Telecommunications Limited, and Help Age. The last group of 20 participants were employees of SMART in Belize City. These organizations stated that providing time for employee screening was beneficial to the health and wellness of the staff. They correlated healthy employees to healthy productivity for the organization. The logistics of taking the screening to the workplace eliminated the need for employee travel to an offsite location. An additional 94 participants were tested, for a total of 130 participants’ data for analysis.
This mixed-method research incorporated a qualitative component that included survey questions related to previous diagnosis of diabetes and patient counseling following results. The quantitative data included waist circumference, blood pressure, and HbA1c measurements. After analysis of the information collected from the pilot study and a literature review of diabetes in Belize, the decision to add blood pressure measurement to future participants was made.
Each participant was given a unique number for anonymity associated with results. Once all results were obtained, participants were provided with a form listing their results and an explanation of the meaning of the results. In addition, each participant met with a Belizean nurse for counseling and answering of any questions related to the results. Participants were informed that referral may be made to a physician for follow-up consulting if necessary. Recommendations and suggestions for diet choices and exercise options were given in both English and Spanish as necessary.
RESULTS
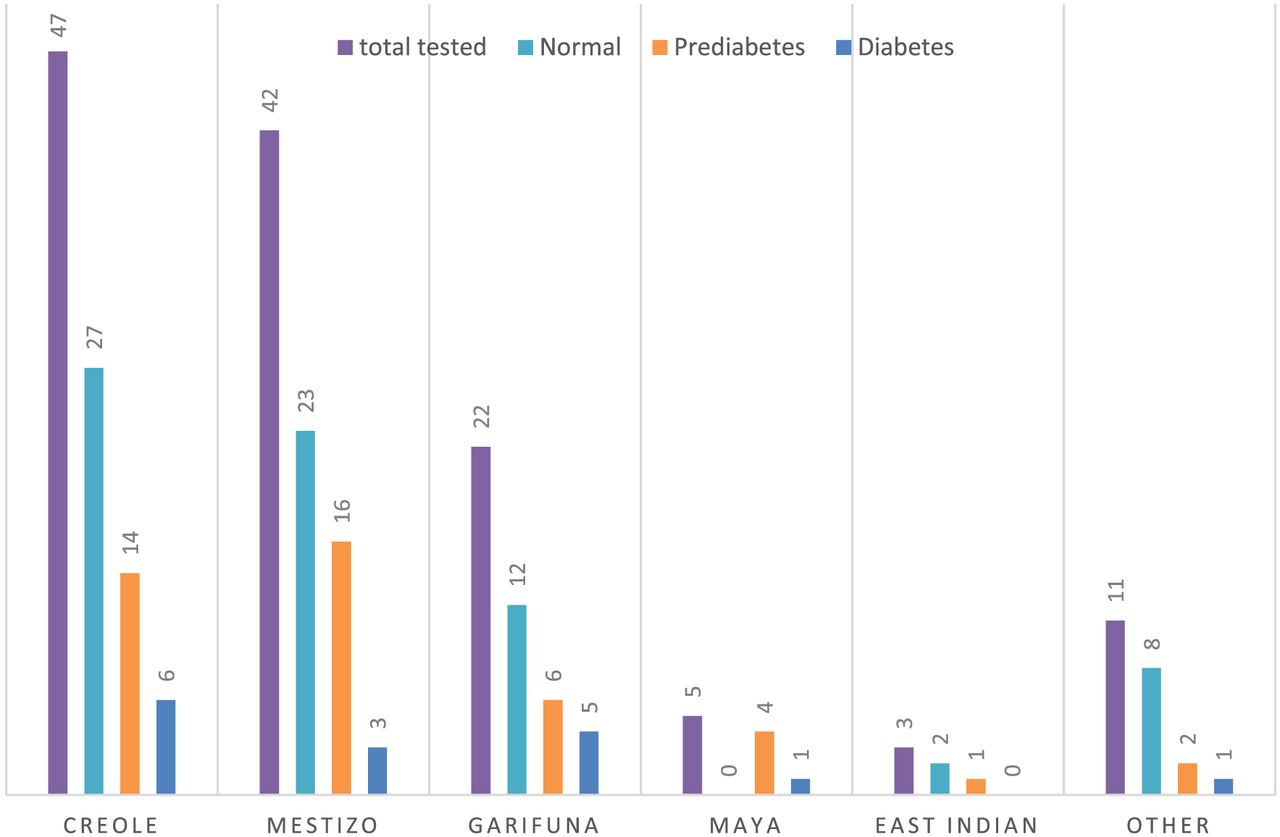
Of the 130 participants tested, 57 (43.8%) were men and 73 (56.2%) were women. Their ages ranged from 20 to 64 years with a mean of 38.2. The highest percent (36.4%) of participants were in the 30 to 39 years age group. Because there are such a variety of ethnic groups in Belize, participants were asked with what group they identify (Figure 2). The largest ethnic group identified as Creole, with 47 participants (36.2%). The next highest number identified as Mestizo, with 42 participants (32.3%), followed by Garifuna with 22 participants (16.9%). There were 5 Mayan (3.8%), 3 East Indian (2.3%), and 11 people (8.5%) categorized in “other,” which consisted of Nigerian, Chinese, Hispanic, and other African ethnicities. As indicated in Figure 2, the highest number of participants with a value in the diabetic range identified as Creole, followed by Garifuna.

Prevalence of diabetes and prediabetes by ethnicity.
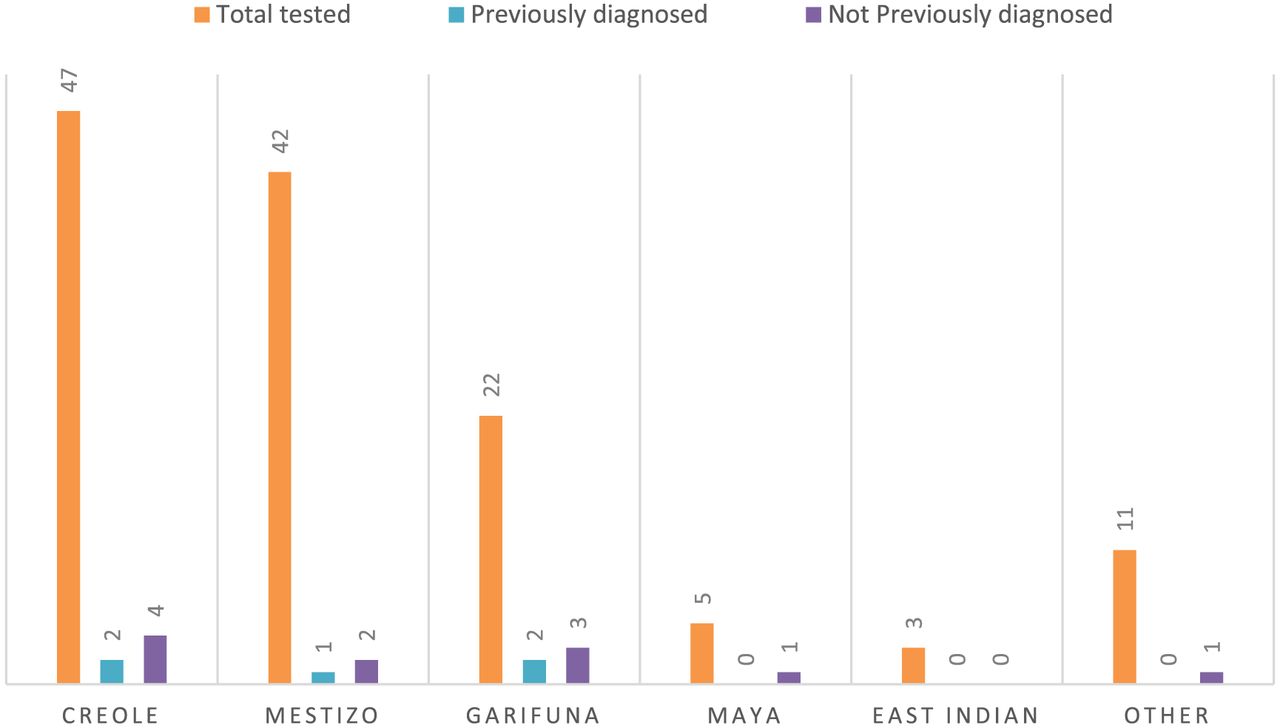
The data collection included a question to participants of whether they had been previously diagnosed as having diabetes. Figure 3 shows the number of participants who had been previously diagnosed as having diabetes was quite small 5 (3.8%) when compared with the 16 participants falling into the HbA1c diabetic range (12.3%). The number of participants with HbA1c in the prediabetic range was 43 (33.1%), confirming the need for education on lifestyle changes for preventing prediabetes from becoming diabetes.

Prevalence of diabetes by previous diagnosis.
A series of analyses of variance (ANOVA) tested whether any of the dichotomous variables, such as gender and previously diagnosed diabetes, or continuous variables, such as age, waist measurement, HbA1c result, or blood pressure measurements, differed based on ethnicity. The findings indicated that none of these variables differed significantly based on ethnicity. A second series of ANOVA were used to determine whether any of the dichotomous or continuous variables differed significantly with identification of normal, prediabetic, or diabetic status based on HbA1c levels. The means of age, waist measurement, and previous diagnosis of diabetes differed significantly.
The mean waist circumference was 38 in. There was a significant correlation between waist circumference and gender, age, and HbA1c levels. Women had lower waist scores than men, and older participants were more likely to have higher waist circumferences and HbA1c levels. Another significant correlation was that older participants were more likely to have been diagnosed with diabetes than younger participants. Because hypertension is an associated concern with diabetes, blood pressure scores were included in the second data collection set. Participants who were diagnosed as having diabetes did have elevated diastolic and systolic blood pressure values, as expected. The statistical analysis did include one blood pressure systolic measurement of 226, which should be considered an outlying data point.
When looking at the correlation of data, 3 diagnostic classifications were used based on the HbA1c measurement: namely normal, prediabetes, or diabetes. The normal group included all participants with HbA1c values equaling less than 5.7% (<39 mmol/mol); the prediabetes group included all participants with HbA1c ranges between 5.7% to 6.4% (39 to 46 mmol/mol); and finally, any participant with an HbA1c value more than 6.5% (>48 mmol/mol) was included in the diabetic group. These data were then correlated with ethnicity to answer the research question of whether any ethnic group was at higher risk. Some participants fell into the diabetic range of those whom had never been diagnosed. One of the goals of this project was to identify participants in the prediabetic range who could benefit from changes in diet and activity.
DISCUSSION
Aviles-Santo et al13 report on the differences in HbA1c values for Hispanic versus non-Hispanic people in Central America, South America, Cuba, and Mexico. This national health and nutrition survey did not focus on any particular country in Central America and did not suggest intervention methods based on cultural diversity. Gulley et al14 describe an occupational diabetes screening program at a major corporation in Belize, the cultural considerations needed when advising participants of their glucose results, and the significance of the findings. Because the typical Belizean diet consists of rice, tortillas, plantains, and fry jacks, patient education on better nutrition sources is important to prevent development of type 2 diabetes. Gulley et al also reflect on the economic issues that contribute to effective or ineffective chronic disease management. Lack of screening tests and medicine to treat diseases contribute to this very important concern in Belize.
This research presents a picture of the prevalence in different groups of people in Belize. Of the 130 participants tested, 72 fell into the normal range for HbA1c and 43 fell in the prediabetes range. A finding of 33.1% of a population with prediabetes values is worth addressing with patient education. Even more concerning is the 16 participants who fell in the diabetes range, with 11 (8.5%) not having been diagnosed previously. Use of patient education materials that address cultural differences will be the next step of this project.
A mixed-methods study by Dekker et al15 presented a needs assessment in Toledo, Belize, an area south of where most of our participants resided. These researchers assessed a patient population for their understanding of type 2 diabetes and hypertension as a means of determining quality of care in country. A common thread among the Gulley study, Dekker study, and the present study is the barrier to care related to financial constraints, transportation difficulties, and, in some cases, inadequate means for daily access to fruits and vegetables. A common conclusion from the studies in Belize is the valuable support provided by employer-promoted health and wellness programs, which ultimately enhance employee performance. For this project, going to the workplace was the ideal method of gaining participation. Partnering with international organizations for funding of supplies to meet the needs of screening an even larger population will be beneficial to the future health outlook for Belize.
The complications resulting from uncontrolled diabetes can be devastating. They include loss of sight, limbs, and kidney function.16 The purpose of the study was to bring awareness and possible intervention to a population who could make changes in diet and activity to prevent advancement to type 2 diabetes. Belize has a rich culture of medicinal plants and their use. Giovannini et al17 have studied the use of medicinal plants used in 7 Central American countries, of which Belize was one. Follow-up studies could also look at the role of medicinal plants growing in Belize that might be useful for diabetes management. Because availability of pharmacological resources is limited, a future study to identify how use of some of these described plant species affect HbA1c values could be extremely beneficial to the people of Belize.
Acknowledgments
All data presented in this article have been collected by the author. The author would like to thank Brad Sagarin for his time on statistical analysis of the data. There is no conflict of interest, and this article has not been published elsewhere.
- Received February 22, 2018.
- Accepted April 7, 2018.
American Society for Clinical Laboratory Science




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.