


This article requires a subscription to view the full text. If you have a subscription you may use the login form below to view the article. Access to this article can also be purchased.
- University of Texas Medical Branch
- University of Texas Medical Branch
- University of Texas Medical Branch
- University of Texas Medical Branch
- University of Texas Medical Branch
- Address for Correspondence: Juan U. Rojo
, University of Texas Medical Branch, jurojo{at}utmb.edu
ABSTRACT
Autoimmune hemolytic anemia (AIHA) is a rare disorder for which epidemiological studies are limited. Proper diagnosis of AIHA is supported by clinical laboratory data that demonstrate all aspects of the disease including evidence of anemia by low hemoglobin (Hb), indication of hemolysis by elevated lactate dehydrogenase, and demonstrating involvement of the immune system by a positive direct antiglobulin test (DAT). The purpose of this study was to investigate the incidence of AIHA at our institution and establish a correlation between DAT strength of reaction and AIHA disease severity. Here, we identified that AIHA is more prevalent among children and patients ages 61 to 70 years old that are female and Caucasian/White Hispanic. A positive correlation between DAT strength and disease severity was observed, and a negative correlation between DAT strength of reaction and Hb was identified. Our findings also showed a positive correlation between age and AIHA type that is dependent on DAT strength. The results from this study propose the further evaluation of DAT as a laboratory value that can indicate severity of the disease and possibly implementing a flag value for DAT when communicating results to clinicians.
- AIHA - autoimmune hemolytic anemia
- DAT - direct antiglobulin test
- Hb - hemoglobin
- ICD - International Classification of Diseases
- LDH - lactate dehydrogenase
- RBC - red blood cell
- wAIHA - warm autoimmune hemolytic anemia
- direct antiglobulin test (DAT)
- autoimmune hemolytic anemia (AIHA)
- hemoglobin (Hb)
- lactate dehydrogenase (LDH)
- epidemiology
- disease severity
- autoimmunity
INTRODUCTION
Autoimmune hemolytic anemia (AIHA) is a rare disease whose epidemiology is not well defined. Studies conducted in Denmark and France estimate the incidence of AIHA at 1.77 per 100 000 individuals and 2.44 per 100 000 individuals, respectively.1⇓-3 This disease is characterized by decompensated acquired hemolysis as the result of the immune system acting against its own red blood cell (RBC) antigens, leading to their destruction.4 The breakdown of RBCs is usually driven by autoantibodies and/or complement that binds to surface antigens and, together with macrophages, T lymphocytes, and cytokines, marks them for removal from the body. AIHA is classified according to serological types depending on the type of antibody involved and temperature phase at which the antibodies react.5 The serological types include warm AIHA (wAIHA), cold agglutinin disease, paroxysmal cold hemoglobinuria, and mixed-type AIHA. There is also a subset of atypical direct antiglobulin test (DAT)-negative AIHA cases.6,7 The disease can be primary, in which diagnosis can only be made when there is no other apparent cause of hemolysis, or it can be secondary due to the presence of underlying disease, such as lymphoproliferative and autoimmune disorders, immunodeficiencies, infections, and tumors. Diagnosis of AIHA is usually confirmed using a combination of laboratory evidence of hemolysis, with demonstration of immune system involvement, and clinically via symptomatic anemia.8 Laboratory evidence of hemolysis is established by the presence of anemia by low hemoglobin (Hb) and indices of hemolysis, mainly elevated lactate dehydrogenase (LDH), haptoglobin, and bilirubin. In clinical practice, these hemolysis indices are usually evaluated prior to performing a DAT. Altogether, they are used to assign an autoimmune involvement to hemolysis with evidence of symptomatic anemia. Indicators of disease severity can aid in prompt intervention for management of the disease. Thus, it would be clinically advantageous to explore whether the DAT value, which is considered the AIHA gold standard laboratory diagnostic test, can also be used as an indicator of disease severity. Several studies have described the diagnostic protocol of AIHA and survival rates of affected patients by assessing their response to therapy.9,10 But to the best of our knowledge, there have not been enough studies, at least in the United States, that have investigated the epidemiology of AIHA, nor have there been any studies aimed at exploring a possible correlation between the strength of DAT and severity of the disease. Being the gold standard for diagnosis, DAT has for the most part been only used as a qualitative test to confirm diagnosis and differentiate serological types. What we do not know is if the strength of DAT by itself can indicate the severity of the disease and if disease severity is varied across different patient demographics. Therefore, this study aims to investigate the demographic distribution of patients diagnosed with AIHA, determine the correlation between strength of DAT and severity of AIHA, and determine if there are any differences in disease severity across patients’ demographics.
MATERIALS AND METHODS
Sample
We performed a retrospective cross-sectional study using patients’ electronic medical records from January 2012 to December 2022 at our institution, which is an 800-bed academic and research hospital that includes 4 campuses and 95 clinics. Data generated from patient visits were entered in Epic, which made data retrieval from any campus and clinic possible. The inclusion criteria required patients who had a diagnosis of AIHA defined by the International Classification of Diseases (ICD)-9 and ICD-10 codes D59.0, D59.1, and 283.0. Laboratory data values included DAT, LDH, and Hb. Clinical data incorporated patient presentation and diagnosis with demographic information that included age, sex, and race/ethnicity. For this study we used a nonprobabilistic purposive sampling model that only included patients diagnosed with AIHA.
Data Analysis and Statistics
IBM SPSS Statistics 28 and Microsoft Excel were used for all data analysis and generation of figures and tables. Pearson correlation coefficient, Spearman’s rho, and Eta11 were used to find statistical significance between variables. Descriptive statistics were used to portray the prevalence of AIHA. Pearson correlation coefficient was used to assess the correlation between age and AIHA severity, whereas Spearman’s rho was used to establish the correlation between DAT and severity. Eta (η) test was used to find the association between 2 variables with one of them being dependent on the other. Eta (η) measures how much of the dependent variable is occurring because of the independent variable, whereas the square of Eta (η2) measured the effect size. Eta was used to evaluate if patient demographics were a contributing factor to AIHA severity. Both Pearson correlation coefficient and Spearman’s tests have correlation coefficients ranging from −1 for a perfect negative correlation, through 0 for no correlation, to +1 for a perfect positive correlation.11
AIHA Severity
An AIHA severity scale was created by combining the LDH and Hb values to generate a score numerical value. Anemia is defined as Hb values <13 g/dL in men and <12 g/dL in women, but as these cutoffs are not always actionable for transfusion support,12 we decided to use the conservative cutoff of 7 g/dL, which is the threshold at which the blood bank would provide transfusion support for nonbleeding symptomatic patients.13 For LDH, all values above the reference range of 200–600 IU/L were considered significant for hemolysis. The combined Hb and LDH values were used to designate a severity score with a scale of 0–2, in which the greater the value indicated increased severity. These values were designated by taking into consideration Hb and LDH values. If both values were outside reference, a severity score of 2 was assigned. If only 1 value, Hb or LDH, was outside range, a severity score of 1 was given, and if both values were within normal range, a severity score of 0 was assigned. Each patient was scored using the values described in Table 1.
AIHA severity score
RESULTS
Cases of AIHA
From January 2012 to December 2022, there were a total of 355 patients diagnosed with AIHA in our study. The mean age was 17.56 years, the median was 2 years, and the modal age was 1 year. From these patients, 47.3% (n = 168) identified as Caucasian/White Hispanic/Latino, 28.7% (n = 102) as Black/African American, 19.2% (n = 68) as Caucasian/White not Hispanic/Latino, 4.5% (n = 16) as Asian, and 0.3% (n = 1) as American Indian/Alaskan Native (Table 2).
AIHA cases by race and ethnicity
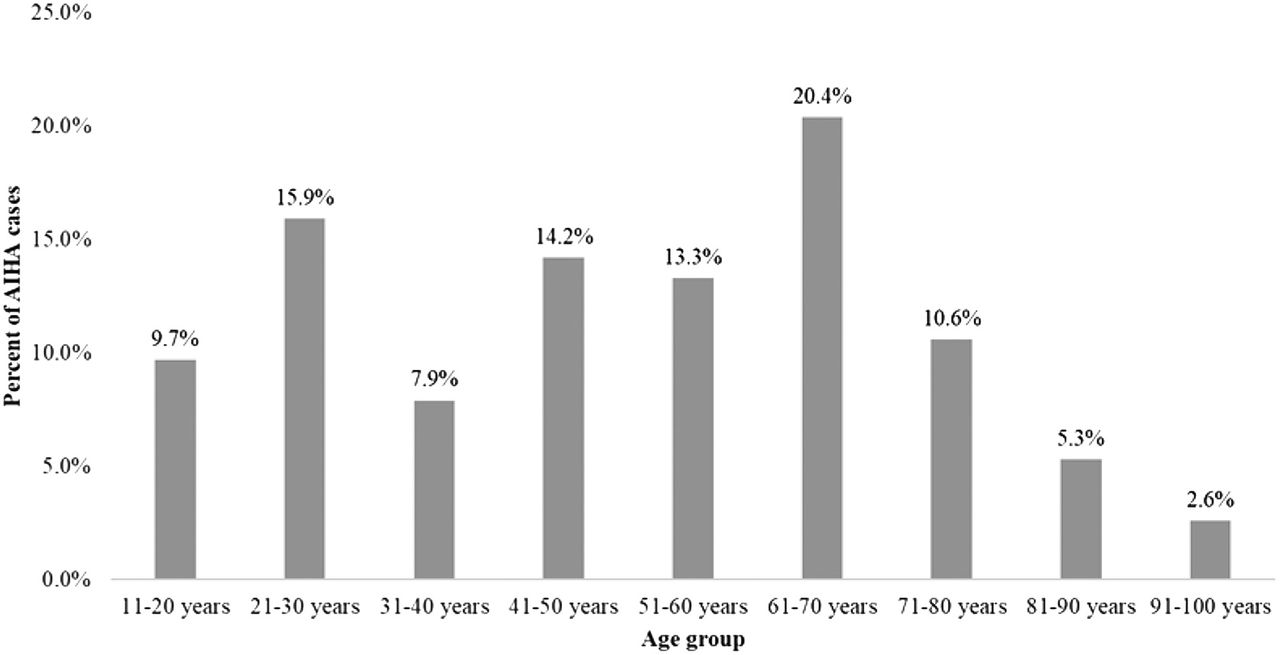
In terms of AIHA incidence by age group (Table 3), it was observed that most cases occurred in the 0–10 years age group, which accounted for 68.2% (n = 242) of patients, whereas the other age groups accounted for 31.8% (n = 113). Male patients accounted for 46.5% (n = 165) of AIHA cases, and female patients accounted for 53.5% (n = 190) (Table 4). The patients in the 0–10 years age group had to be excluded from further analysis as they lacked complete laboratory data values, and analysis only included patients older than 11 years old (n = 98) (Figure 1).
AIHA cases by age group
AIHA cases by sex

AIHA cases by age group older than 11 years old.
Correlation between DAT Strength of Reaction and AIHA Disease Severity
To determine the correlation between DAT strength and severity of AIHA, the severity score depicted in Table 1 was utilized. Only patients with complete laboratory values (n = 98) were analyzed to look for correlations between DAT (polyspecific, IgG, and C3) and LDH, Hb, and severity. Using Spearman’s rho test and statistically significance at P < .01, a positive correlation between DAT polyspecific, IgG, and C3 and severity at 0.364, 0.253, and 0.326, respectively, was found (Table 5). Thus, as DAT strength of reaction increases, so does AIHA severity score. However, this correlation was only statistically significant (P < .01) for DAT polyspecific and C3 severity. A negative statistically significant (P < .01) correlation between DAT result and Hb value at −0.35, −0.280, and −0.361 for DAT polyspecific, IgG, and C3, respectively, was found, but not in the case of LDH, indicating that DAT strength of reaction increased as there was a decrease in Hb value.
Correlation between DAT and LDH, hemoglobin, and severity
AIHA Severity across Patient Demographics
Pearson’s product moment correlation coefficient was used to evaluate for correlation between patient age and AIHA severity. Our data showed a statistically significant (P < .01) positive correlation at 0.441, indicating that increased age is associated with clinical presentation of AIHA (Table 6). Spearman’s Eta statistical test was used to assess the association between sex and race/ethnicity with severity of the disease, which demonstrated little to no association at n = 0.300 and 0.33, respectively, and the effect size was medium for ethnicity (η2 = 0.09) but large (η2 = 0.11) for type of AIHA (Table 7). Our data showed 64% of patients presented with wAIHA, 46% had cold AIHA, and 26% presented unspecified type, which included patients who had a diagnosis of AIHA but with a negative DAT result.
Correlation between age and AIHA severity
AIHA severity by race, sex, and ethnicity
DISCUSSION
AIHA is a rare disease for which epidemiologic data are still needed to fully comprehend the prevalence and affected populations. This is one of the few studies conducted in the United States that investigated the incidence and severity of AIHA. Though limited to our institution, which is predominantly populated by Caucasian and Hispanic individuals, our data are consistent with the ethnicity and racial makeup of the local population. The age distribution identified 68.2% of AIHA cases was found in patients who were 0–10 years of age. However, this group had to be excluded from further analysis because they did not have a DAT performed. After excluding patients younger than 10 years old, it was observed that most of AIHA cases (58.5%) occurred in patients between the ages of 40–80 years old. This age disparity is consistent with other studies that suspect AIHA to be the result of underlying conditions, mainly autoimmune and lymphoproliferative diseases common in this age range.14,15 In agreement with previously reported data, we found the majority of AIHA cases to occur in female patients.2,16,17 Proper diagnosis of AIHA involves demonstration of all aspects of the disease.18,19 This means there must be presence of anemia (low Hb), evidence of hemolysis (elevated LDH), and immune system involvement (positive DAT). Using the AIHA severity score that we generated, it was observed that as DAT strength of reaction increases, so does the AIHA severity score. Similar findings were reported when the relationship between in vivo hemolysis and strength of DAT, type of RBC-bound immunoglobulin, and IgG subclass.16 However, their study was prospective in design, whereas our current study is retrospective. To the best of our knowledge, this is the first time a statistical significance has been assigned to the relationship between AIHA severity and DAT strength. This relationship was further evaluated, and a negative statistically significant correlation between DAT and Hb value was found, but not for LDH. This indicates that as the DAT strength of reaction increases, there is a decrease in Hb value. This is consistent with AIHA severity in which patients present with anemia and increased RBC damage. Interestingly, although not statistically significant, our data suggest a negative relationship between monospecific DAT IgG/C3 and LDH. Hemolysis of RBCs can be intravascular or extravascular, IgG-coated RBCs are removed from circulation by the spleen, and if there is delayed compensation by the bone marrow, anemia ensues before these cells have the time to hemolyze due to C3 coating them.20 This helps explain the negative relationship between DAT and Hb observed in our data. Regarding the correlation between patient demographics and AIHA severity, our findings showed a positive correlation indicating that increased age is associated with AIHA. This is suggestive of AIHA as the result of comorbidities such as diabetes and cardiovascular disease that are commonly present in patients this age group.21 Thus, we suspect that secondary AIHA is a contributing factor in this relation between age and severity. Surprisingly, there was little to no association between sex/race and severity. However, ethnicity and AIHA type showed moderate association, and the effect size was medium for ethnicity but large for type of AIHA. Many of our patients presented with wAIHA followed by cold AIHA and unspecified type. The unspecified category reported in our data denotes patients diagnosed with AIHA but who had a negative DAT result. This finding is consistent with previous studies that have reported a small percentage of negative DAT AIHA cases.4,22⇓-24 In those studies, it was reported that the negative DAT was either due to sensitivity of the test method that was used or that the test system was not designed to detect the type of offending immunoglobulin. Also, wAIHA has been reported to be the most common and usually severe type of AIHA, accounting for close to 65% of all patients with AIHA,25,26 which is consistent with our data. Overall, this study seeks to continue collaboration between clinicians and laboratory specialists to provide additional information that can be used in disease diagnosis and management.27 As an example, other studies have utilized DAT values to predict the need for phototherapy in newborns and used them to predict hyperbilirubinemia in infants.28⇓-30 One of the major limitations of our study is the unavailability of laboratory data from patients under the age of 10 years old, as Hb and LDH values were missing. Also, our analysis depended on secondhand data collected for diagnostic and medical record purposes. Finally, our study is limited to the patient population admitted at our institution; thus, a more comprehensive study should be completed.
CONCLUSION
This is one of the few studies available that investigates the epidemiology of AIHA. To the best of our knowledge, this is the first study that demonstrates an association between DAT strength of reaction and severity of AIHA. We created a scale to grade AIHA severity based on Hb and LDH values as well as demonstrated that AIHA severity increases with age in patients over 10 years old and is type dependent. With knowledge and statistically suggestive evidence of DAT being an indicative factor of AIHA severity and the presence of a strong association between AIHA type and AIHA severity, it supports the concept of implementing a mechanism to alert a critical value for DAT in the context of diagnosing AIHA. This would help prompt immediate and tailored treatment in real time as per communication between the testing laboratories and the clinicians.
CONFLICTS OF INTEREST
All authors declare no conflict of interest.
FUNDING
This research received no external funding.
INSITUTIONAL REVIEW BOARD STATEMENT
Our Institutional Review Board (IRB) reviewed this study and determined the project to be a quality assessment/quality improvement study that met the criteria for exemption from review or oversight (IRB #23-0025).
ACKNOWLEDGMENTS
The authors would like to thank the Clinical Laboratory Sciences Department faculty and staff at the University of Texas Medical Branch for their continued support.
- Received July 11, 2023.
- Accepted December 19, 2023.
American Society for Clinical Laboratory Science
REFERENCES




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Keywords
- AIHA - autoimmune hemolytic anemia
- DAT - direct antiglobulin test
- Hb - hemoglobin
- ICD - International Classification of Diseases
- LDH - lactate dehydrogenase
- RBC - red blood cell
- wAIHA - warm autoimmune hemolytic anemia
- direct antiglobulin test (DAT)
- autoimmune hemolytic anemia (AIHA)
- hemoglobin (Hb)
- lactate dehydrogenase (LDH)
- epidemiology
- disease severity
- autoimmunity