


This article requires a subscription to view the full text. If you have a subscription you may use the login form below to view the article. Access to this article can also be purchased.
- Alaska Regional Hospital Laboratory, Anchorage, Alaska
- Department of Research Programs, Fort Belvoir Community Hospital, Fort Belvoir, VA
- Department of Biomedical Laboratory Science, School of Medicine and Health Sciences, The George Washington University
- School of Systems Biology, George Mason University
- Address for Correspondence: Yuliya Dobrydneva
, School of Systems Biology, George Mason University, yuliyad757{at}gmail.com
ABSTRACT
INTRODUCTION: Erythrocyte sedimentation rate (ESR) and high-sensitivity C-reactive protein (hs-CRP) are screening tests for inflammation and are often ordered simultaneously. Our study investigated concordance between ESR and hs-CRP to optimize patient diagnosis.
METHODS: A retrospective review was conducted on ESR and hs-CRP tests performed simultaneously in the same clinical encounter during a 10-month period at Alaska Regional Hospital. Kappa statistics and correlation coefficients were calculated to evaluate the level of concordance between ESR and hs-CRP tests. Logistic regression models and receiver operator characteristic (ROC) curves were constructed to evaluate the ability of each screening test to predict the other screening test.
RESULTS: ESR and hs-CRP were elevated in 54% and 76% of the patient population (N = 860) respectively. Among patients with abnormal ESR, 93% also had abnormal hs-CRP, whereas among patients with abnormal hs-CRP, 66% also had abnormal ESR. ESR and hs-CRP tests agreed in 70% of cases. Kappa statistics indicated a fair to moderate level of agreement between dichotomous ESR and hs-CRP tests, with significant differences among patients with and without noninfectious organ diseases, but no other demographic or clinical characteristics. The correlation coefficient between continuous ESR and hs-CRP was nearly 0.40, with no statistically significant correlation among patients with connective tissue/musculoskeletal/autoimmune diseases or diabetes. Finally, hs-CRP and ESR were predictive of each other based on logistic regression and ROC analyses.
CONCLUSION: hs-CRP identified the majority of inflammatory conditions and should be included in the first line of testing when the clinical indication clearly suggests an inflammatory process.
- AUC - area under the curve
- CI - confidence interval
- ESR - erythrocyte sedimentation rate
- Hs-CRP - high-sensitivity C- reactive protein
- LIS - laboratory information system
- RA - rheumatoid arthritis
- RBC - red blood cell
- ROC - receiver operator characteristic
- SLE - systemic lupus erythematosus
INTRODUCTION
Acute phase reactants are proteins produced by the liver when the body experiences inflammation due to infection, injury, or trauma. Two laboratory tests often ordered simultaneously to detect these acute phase reactant proteins are erythrocyte sedimentation rate (ESR) and high-sensitivity C-reactive protein (hs-CRP). While the 2 tests offer a multifunctional approach to detecting and monitoring the inflammatory reaction for patients with various diseases and conditions, results are often contradictory, causing confusion and frustration among physicians. By combining results from ESR and hs-CRP in conjunction with other laboratory data and diagnostic information, physicians can gain insight into potential disease factors.1 A study conducted by Kainth and Gigliotti demonstrated the CRP assay has a 95% sensitivity, while the combined ESR and CRP testing only increased the sensitivity by 3%.2 There has been much debate surrounding the causes of ESR and CRP discordance, but there is limited guidance on the use and interpretation of these tests. Thus, clinically, it is important to understand the role of these screening tests in the detection of inflammation.
ESR, an indirect measurement of the acute phase reactants, is correlated with elevated levels of the coagulation protein fibrinogen and, to a lesser extent, α2-, β-, and γ-immunoglobulins because of the viscosity of these proteins in the plasma affecting the rate at which the red blood cells (RBCs) settle.3 These proteins decrease the RBCs’ zeta potential to promote the formation of rouleaux, which sediments more rapidly than single cells, yet responds to inflammatory acute phase reactants very slowly if not at all when the inflammation is minor.4 The gradual 24–48-hour initial response and extensive elevation to an inflammatory reaction is the result of the “long half-life of some plasma proteins and perhaps to a longer amplified response time.”1 ESR is especially useful for diagnosis and monitoring of the autoimmune conditions polymyalgia rheumatica and temporal arteritis. Factors that limit the ESR result interpretation in clinical practice include increased anticoagulant to blood ratio; position, placement, or vibration of sedimentation tube; and RBC size (microcyte vs macrocyte) and shape (normal vs sickle cells or spherocytes). Other factors that also limit these results are cell number (anemia vs polycythemia) or bubbles in the RBCs, abnormal protein and immunoglobulins levels, or systemic comorbidities such as autoimmune diseases or renal insufficiency.3 These confounding factors lead to difficulties in determining a reference interval for patients. Although reference intervals vary among medical facilities, currently, reference intervals are characterized by the patient’s gender and age. Typically, the reference interval for a male patient is calculated by dividing the age in years by 2 while a female patient’s reference interval is calculated by adding 10 to her age in years.1 Men typically have a lower reference interval than women considering the hormonal, weight, and metabolic changes experienced by women with increased age, pregnancy, or menses.1
The hs-CRP, a pentameric protein, is used to identify foreign pathogens and damaged cellular debris resulting in the activation of the complement pathway and phagocytosis.3 The levels of this nonspecific diagnostic inflammatory marker increase within 4–6 hours of tissue injury with the release of signaling cytokines, “allowing for rapid clearance after a source of inflammation is resolved.”5 The hs-CRP levels can double every 8 hours with peak levels seen at 36–50 hours of inflammation, and subsequently levels are expected to fall rapidly as inflammation subsides, giving physicians a real-time assessment to the level of inflammation.6 Utilizing the plasma or serum from a routine blood sample can yield results within 15–30 minutes, depending on the laboratory analyzer. False test results are only seen in patients with hepatic failure since the proteins are produced in the liver. The hs-CRP test’s analytical sensitivity can quantify amounts of CRP as small as 0.1 mg/L to assess the risk of an inflammatory reaction process much sooner than CRP.
The purpose of this study is to investigate the level of agreement and correlation between the 2 markers of systemic inflammation, namely ESR and hs-CRP, obtained in a clinical setting. Furthermore, this study examined underlying factors that may lead to concordant or discordant test results, allowing physicians better choices for the patient without creating uncertainty or increasing expenditure in the clinical environment.
METHODS
Study Design
A cross-sectional study was conducted at Alaska Regional Hospital, a general medical and surgical facility in Anchorage with 250 acute care beds. The hospital has a modernized laboratory information system (LIS) with a comprehensive list of test order sets, laboratory results, hospital reports, and discharge diagnoses within the patient’s electronic medical record, referenced by hospital encounters and admission dates. A retrospective review of medical records that included ESR and hs-CRP tests performed simultaneously in 1 clinical encounter over a 10-month period was conducted.
Participants
Medical records of patients admitted to the emergency department, inpatients, and outpatients with at least 1 ESR and 1 hs-CRP result recorded on the same date between November 2018 and September 2019 were included. A patient may have had multiple ESR/hs-CRP tests during 1 hospital stay or multiple hospital visits within the time frame studied. Including the first or last test results would bias the results of this analysis, leading to inconsistent findings considering the ESR’s languid rise and fall.7 Consequently, only 1 simultaneous ESR and hs-CRP order per patient was selected at random using Microsoft Excel, and those with duplicate orders or multiple hospital encounters were excluded. Patient age, biological sex, and diagnoses results were recorded from the LIS, and patient charts were reviewed for conditions known to have an impact on ESR levels. Since fibrinogen and globulin levels are already elevated in pregnant women, resulting in elevated ESR levels during pregnancy, we excluded pregnant women from the study sample.6 Sickle cell or anemic patients were also excluded from the study sample because ESR levels could be artificially reduced due to slow settling of abnormally shaped RBCs. Data obtained from patient diagnoses were classified into 7 broadly defined disease states (malignancy, connective tissue/musculoskeletal/autoimmune, noninfectious organ diseases, colitis/enteritis/other inflammatory conditions, pericarditis/endocarditis, diabetes, mixed comorbidities) to associate a single indication for ESR/hs-CRP testing when multiple indications were found.
Procedures
Both ESR and hs-CRP measurements were performed in the hospital clinical laboratory accredited by the College of American Pathologists. ESR was measured using the Wintrobe tube method. Approximately 1 mL of well-mixed EDTA venous whole blood was drawn up into the tube using the pipette bulb until the cotton plug was entirely saturated. The erythrocytes settled vertically out of the venous plasma toward the bottom of the tube. Sample results were read after 60 minutes at the plasma/red cell interface on the 0–100 mm graduated tube. The Siemens Healthcare Diagnostics Dimension EXL analyzer was used to assay the hs-CRP levels by detecting the agglutination of CRP from heparinized serum or plasm and the CRP monoclonal antibody. Absorbance at 405 and 510 nm was used to measure change in agglutination. To maintain instrument accuracy, calibrations were performed every 90 days for ensuring an analytical measurement reference interval of 0.1–15.0 mg/L.
Statistical Analysis
Demographic, clinical and laboratory data were analyzed using SAS version 9.4 (SAS Institute, Cary, NC). Demographic data included biological sex (male, female) and age (years) while clinical data included indicator variables to classify patients according to presence or absence of comorbidities. Laboratory data included ESR and hs-CRP results defined as continuous variable (in mm/hour for ESR and in mg/L of hs-CRP) and as a dichotomous variable (abnormal vs normal) based on predefined reference intervals. Dichotomous ESR and hs-CRP variables were cross-tabulated, and kappa statistics with their 95% confidence intervals (CIs) were calculated as estimates of agreement between these 2 laboratory tests, before and after stratifying by demographic and clinical characteristics. We used stratified kappa statistics and examined overlap in their 95% CI to assess significant differences in agreement between ESR and hs-CRP variables according to demographic and clinical characteristics. Similarly, Pearson’s correlation coefficients were calculated for continuous ESR and hs-CRP tests, before and after stratifying by demographic and clinical characteristics. Logistic regression models and receiver operator characteristic (ROC) curves were constructed, whereas continuous hs-CRP was included as a predictor of dichotomous ESR and vice versa in order to estimate the area under the curve (AUC) for a continuous laboratory test as a predictor of a dichotomous laboratory test. Kappa statistics can be interpreted as follows: k ≤ 0 (no agreement), 0.01–0.20 (slight), 0.21–0.40 (fair), 0.41–0.60 (moderate), 0.61–0.80 (substantial), and 0.81–1.00 (almost perfect) agreement. By contrast, there are no prespecified cutoff points for Pearson’s correlation coefficients, which can range between −1 and +1. However, there is consensus that the closer the value of the correlation coefficient to zero, the weaker the linear relationship between 2 continuous measures. Similarly, an ROC AUC >0.50 suggests that the continuous measurement is predictive of the dichotomous measurement.
RESULTS
A total of 860 patients (440 men and 420 women) from patient records were identified as being study eligible, with a mean (±standard deviation) age of 52.55 (±17.36) years; 43.6% of patients were classified as having mixed comorbidities, while 2.8% were classified as having a malignancy, with prevalence rates of other health conditions ranging between 3.3% and 32.8% (Table 1).
Demographic and clinical characteristics of patient population (N = 860)
As seen in Table 2, the ESR and hs-CRP comparison indicates a strong correlation between the 2 variables, indicating that abnormal results on one assay will lead to abnormal results on the other assay. The normal results for both assays are consistent as well. Table 3 demonstrates that hs-CRP and ESR tests were in fair to moderate agreement with an estimated kappa statistic of 0.38 (95% CI: 0.32-0.43), with no significant differences in kappa statistics based on gender, age group, or comorbid conditions, except for noninfections organ diseases.
Cross-tabulation of hs-CRP and ESR test results
Kappa statistics with 95% CIs for dichotomous ESR and hs-CRP
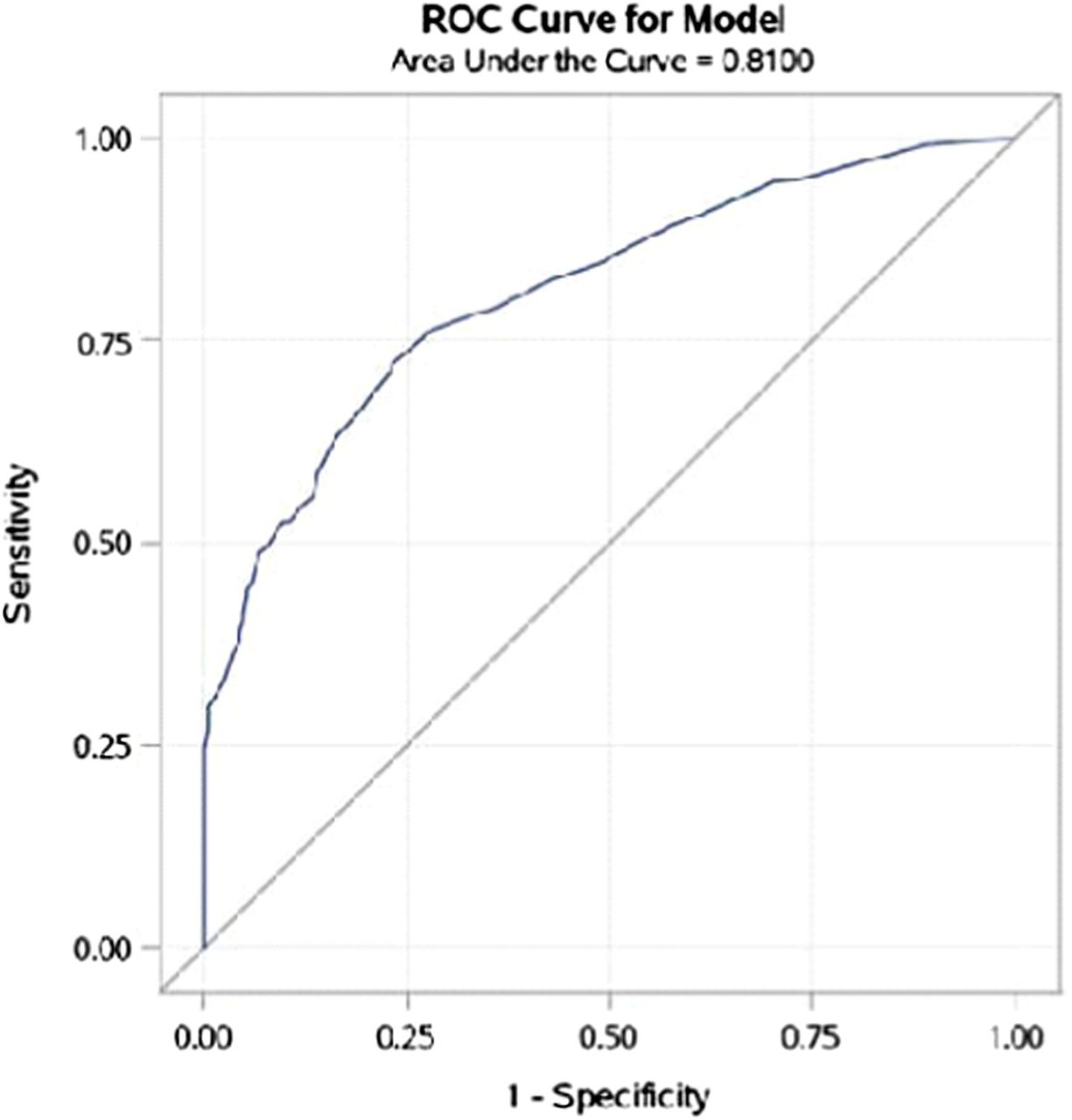
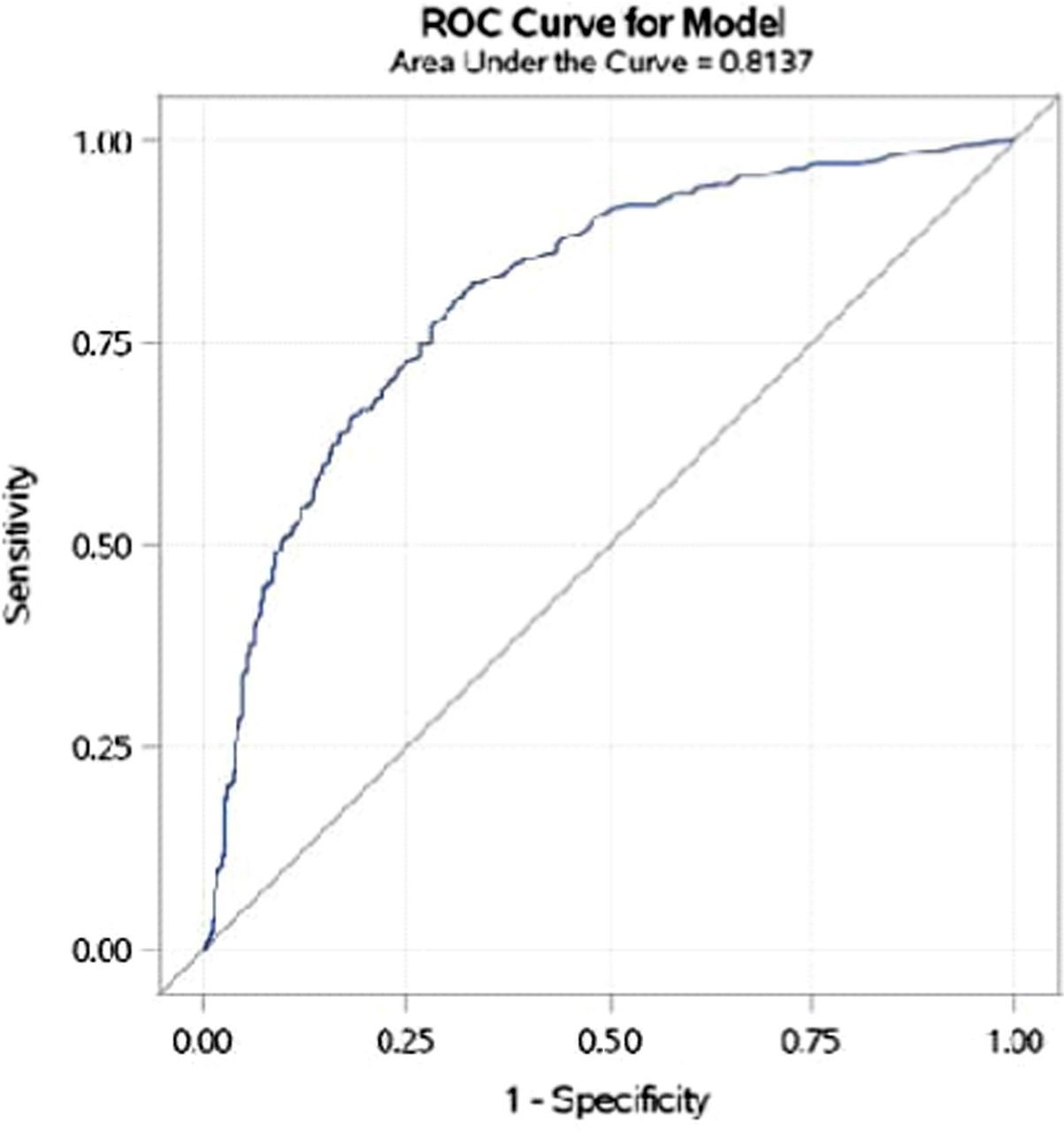
According to Table 4, the estimated Pearson’s correlation coefficient for the association between ESR and hs-CRP, measured on a continuous scale, was estimated to be 0.43 with minor differences according to gender. Correlations among these laboratory measurements also varied according to the health conditions listed in the table and were statistically significant across all conditions except for connective tissue/musculoskeletal/autoimmune diseases and diabetes. Based on results of logistic regression and ROC curves, the AUC for ESR as a predictor of hs-CRP was 0.810, suggesting hs-CRP can predict ESR and vice versa (Figures 1 and 2).
Correlation coefficients for continuous ESR and hs-CRP

ROC curve for hs-CRP as predictor of ESR.

ROC curve for ESR as predictor of hs-CRP.
DISCUSSION
In this retrospective study, a fair to moderate level of agreement was observed between dichotomous ESR and hs-CRP laboratory tests, with significant differences in kappa statistics among patients with and without “noninfectious organ diseases,” but no other characteristics. Similarly, Pearson’s correlation coefficient between continuous measures of ESR and hs-CRP was approximately 0.40, with slight variation according to subgroups defined by demographic and clinical characteristics and no statistically significant correlations among patients with connective tissue/musculoskeletal/autoimmune diseases or diabetes. Finally, hs-CRP and ESR were predictive of each other based on AUC derived from ROC curves.
Our results demonstrated that ESR was elevated in 54% of patients, whereas hs-CRP was elevated in 76% of patients. Both markers were elevated in 50% of all reviewed cases. Among patients with abnormal ESR, 93% also had abnormal hs-CRP, whereas among patients with abnormal hs-CRP, 66% also had abnormal ESR. Accordingly, hs-CRP testing is likely to identify the majority of patients with inflammatory disease that would have been identified using ESR testing but not vice versa, explaining the modest level of agreement and correlation between these 2 laboratory measurements. In addition, these results indicate that hs-CRP can be used alone to identify most cases of inflammatory disease.
Prior studies have assessed the relevance of ESR/hs-CRP measurement for the diagnosis or monitoring of inflammatory diseases. Sbong and Feldman analyzed both markers in 70 patients, indicating discrepancies between the 2 markers could be explained by the delayed rise and fall of the ESR.8 However, a strong correlation (0.6944) between ESR and CRP test results was found in 200 patients with rheumatic diseases.9 In a United Kingdom cohort study of 136 961 patients, CRP had higher sensitivity and specificity than ESR, though both tests had poor diagnostic accuracies (AUC CRP 0.617 vs ESR 0.589, P < .001).10
This study demonstrated that the ESR and hs-CRP test results agreed in approximately 70% of cases reviewed, suggesting that the more sensitive hs-CRP test is adequate on its own for most clinical indications. However, it is important to note that certain disease states are better monitored with one inflammatory marker over the other. Similar to other studies, this study indicates that hs-CRP is the better prognostic marker for infections and sepsis when the procalcitonin test is not available in the laboratory. Studies involving patients with infective endocarditis and patients with sepsis and septic shock showed CRP was prognostically superior to ESR.11 In contrast, patients with autoimmune connective tissue disease exacerbations such as systemic lupus erythematosus (SLE) or rheumatoid arthritis (RA) did not benefit from hs-CRP test results unless an active bacterial infection was present. It is hypothesized that patients with active SLE flare-ups either have a decreased production or increased clearance of CRP, thereby making the hs-CRP results appear normal.12 While RA patients have prolonged joint inflammation, the slow rise and fall of the ESR test would be a better indicator of inflammation to use for monitoring purposes.
Creative and innovative efforts to reduce healthcare costs are at the forefront of economic debates. Hospitals target laboratories to control expenditures while maintaining patient safety and test quality. Meidani et al performed a pilot study of 50 randomly selected medical records to assess laboratory test utilization’s appropriateness and concluded that 26.4% of test requisitions with ESR were inappropriate based upon the patient’s signs and symptoms.13 An ESR/CRP co-ordering study conducted by Juskewitch et al concluded an annual savings of $320 000 when an electronic health record support rule was installed in the LIS to recommend CRP testing over ESR for undiagnosed patients suspected of inflammation.5 Similarly, the intervention aimed to reduce inappropriate coutilization of hs-CRP and ESR yielded a monthly 33% decrease in ESR utilization and 25% reduction in combined hsCRP and ESR utilization.14 Therefore, the management of discordant ESR and hs-CRP measurements can be simplified with test ordering culture change.
Strengths and Limitations
This study highlights the importance of national electronic record guidelines that physicians need when screening and monitoring patients for inflammation. Physicians evaluate numerous patients on a daily basis, resulting in difficulties in maintaining a subjective evaluation for each patient, resulting in ordering a battery of unnecessary tests. A limitation of this study is that the data were gathered during the winter months in Alaska. Alaska is known for its high prevalence of unhoused and drug-using population, potentially impacting acute phase reactants and posing increased comorbidities. Two key confounding variables are the older age of participants and the collection of 1 hospital’s data in this study. It would have been desirable for other local hospitals to contribute data towards this study.
CONCLUSION
ESR and hs-CRP tests are good markers for monitoring inflammation in conjunction with more specific biomarkers; however, this study suggests that a modest level of concordance exists between these 2 markers of inflammation and that hs-CRP can by itself identify the majority of inflammatory disease cases. Thus, the more sensitive hs-CRP test should be utilized as the first line of testing over the ESR when the clinical indication clearly suggests an inflammatory process. The potential pitfalls of an ESR test due to confounding factors such as hemoglobinopathies, systemic vs specific disease states, anticoagulant to blood ratio, tube position and movement, and increased age should be considered while prescribing the test.15 The “Choosing Wisely” initiative promotes the use of the more sensitive hs-CRP test for the screening of acute inflammation contributing to higher quality of care, cost-effective implementation of diagnostic services, and effective use of laboratory resources and personnel in order to streamline testing in lieu of tradition.16
ACKNOWLEDGEMENTS
DISCLAIMER: The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Fort Belvoir Community Hospital, Defense Health Agency, Department of Defense, or US Government. Any discussion or mention of commercial products or brand names does not imply any endorsement by the Federal Government.
ETHICAL APPROVAL: This research activity was determined to be exempt from the Alaska Regional Hospital Institutional Review Board in accordance with current regulations and institutional policy.
RESEARCH FUNDING: None.
COMPETING INTERESTS: None.
- Received March 27, 2024.
- Accepted May 1, 2024.
American Society for Clinical Laboratory Science
REFERENCES




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Keywords
- AUC - area under the curve
- CI - confidence interval
- ESR - erythrocyte sedimentation rate
- Hs-CRP - high-sensitivity C- reactive protein
- LIS - laboratory information system
- RA - rheumatoid arthritis
- RBC - red blood cell
- ROC - receiver operator characteristic
- SLE - systemic lupus erythematosus
- erythrocyte sedimentation rate
- high-sensitivity C-reactive protein
- inflammation